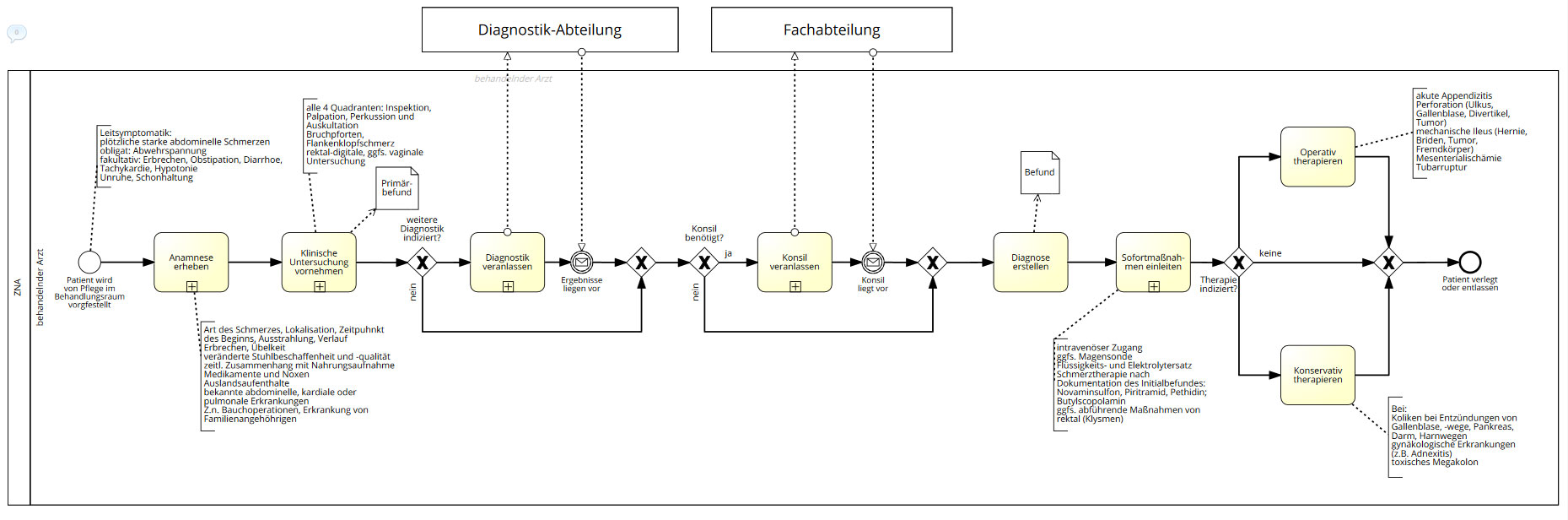
Of course it doesn’t hold up in reality: The first two tasks in the heat of the moment basically merge into each other, are done in parallel. The last single task (“Sofortmaßnahmen einleiten”) basically is done whenever indicated (and consists of several distinct activities anyway). The two tasks with the external pools also aren’t that clear cut and may cross-over. In short: A typical knowledge worker situation. Hence I am trying to model the same situation in CMMN:
This is my first “real” CMMN model and somehow I get stuck (there is not much information on how to do “real” as in “not underwriting or doing something in a cushy chair at the desk stuff” CMMN model to be found, I guess).
I presume that I am not getting my mind to think in the right dimensions - BPMN is relatively easy. What I am having problems with is modelling cause and effect:
Unclear diagnosis? Get more diagnostics. Get advice from a colleague. Still not enough? Evaluate. Set a division the case belongs to. Get rid of the patient by transferring him/her there. Many more patients pressung through the door? Transfer the patient as soon as possible.
I know this sounds like a mess, but right now I don’t know where my next step is.
My “experience” is, that there is few if any advanced literature on how to model more involved CMMN models, especially in healthcare, in fact, there is pretty much Freund/Rücker and the spec and nothing else.
Ive wrestled with best practice myself. There seems to be large body of knowledge re BPMN, however CMMN is still in the pioneering phase. For what its worth, I examine your models with a keen interest…
Thanks for the reply - in that case I’ll post my other models as well (still in the making). Apart from doing the modelling in CMMN, you also have a huge grey area where you can combine the two notations - making things even more confusing.
With that being said, I hiighly recommend you to mix case management and bpmn through call of activities to make the distinction between correlated steps and those wiith “more flexibility”
Thanks for the link - that’s the English version of the Freund/Rücker book I mentioned, though.
Yes, I am currently modeling a few of the medical processes in the ED and in the end it amounts to a mix of BPMN and CMMN (with a sprinkle of DMN). The trick is to know where to switch - and then how to model CMMN. It feels pretty much like having to invent the wheel.
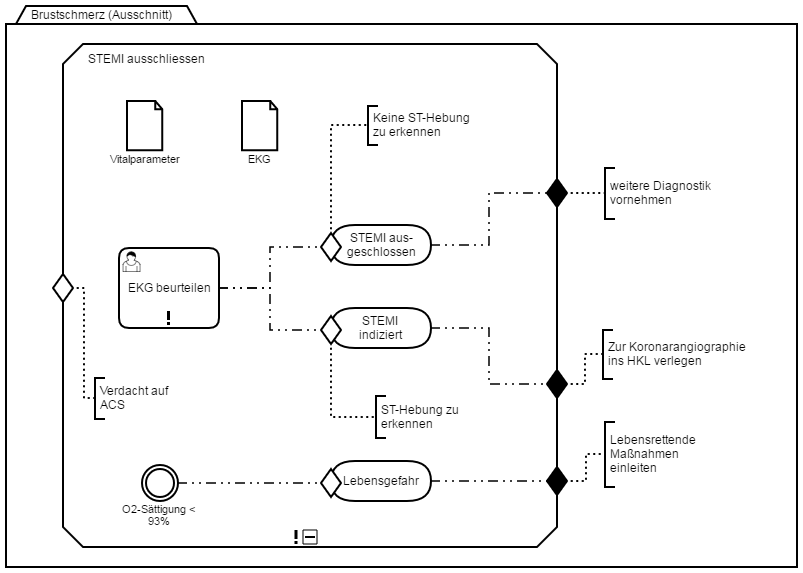
This is one of my most basic examples - not an entire process but rather just one stage in the diagnostic process to confirm or rule out ACS (cardial infarction).
As file documents I do have vital parameters and the results of the electrocardiogram. All you do (mandatory) is judge the electrocardiogram and look for a raised ST-area in it. If you see it, a STEMI is diagnosed and you rush the patient into the coronary operating theatre (middle exit).
Otherwise you exit the stage to do more diagnostics (upper exit).
If at any point the O2 concentration dips below 93% you exit the diagnostiscs and go straight into life-saving mode (lower exit).
That sounds reasonably semantically correct, I do not know though how you would make an executable model out of it (nor even if it is your intent to make up an executable model). But in any case, I don’t seem to detect the necessity for CMMN here, it seems to me like a straight forward BPMN example!
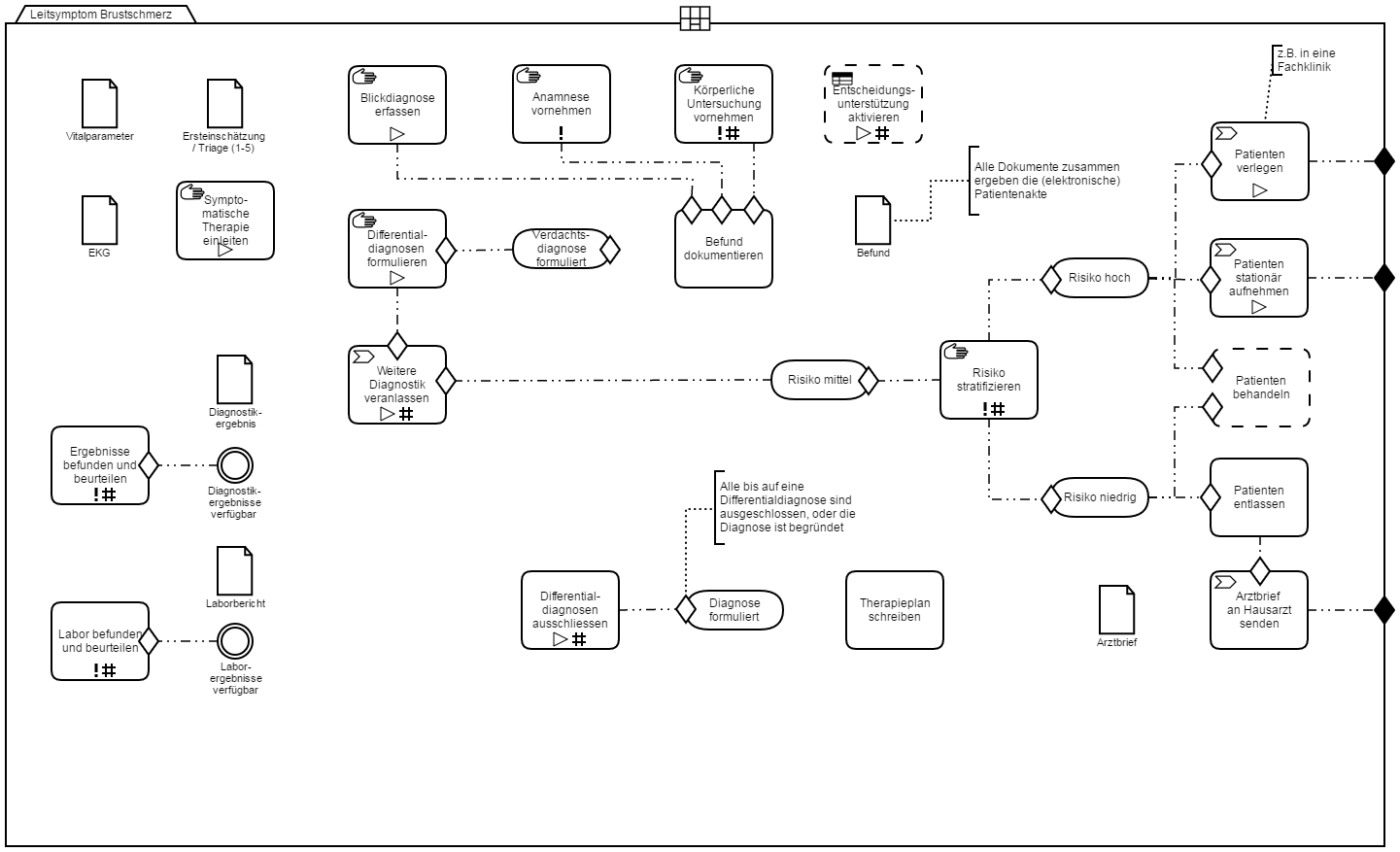
Now, this one is (in theory) the entire process to go through for a patient presenting himself with chest pain. What I haven’t thought through yet, is how to integrate the process to confirm or rule out the possible causes (for now I represented this in the action “Differentialdiagnosen formulieren” which which then leads to 1…n instances of the following activity “Weitere Diagnostik veranlassen”. Basically those should trigger several clinical pathways/SOP, which in turn are interdependent (obviously a lab report you do for one, you can use for the other as well, as an example).
At risk of necro-bumping an old thread, I wanted to check in to see if you are still heading down the path of using CMMN. We really like the concept, conceptually, but haven’t taken it to implementation. I’d love to hear how things are progressing.
For us, BPMN on its own is producing overly long and complicated flows. To give a bit of context, we are in the process of automating care plans for chronic conditions including diabetes, mental health and heart health. Our focus is more on driving behavior change and self-management over longer periods versus diagnosis and immediate interventions - forgive my lack of German, but my understanding is that your use-case might be more about immediate interventions.
If it helps, our plan is to put algorithms behind CMMN sentries to trigger a series of optional “Next Best Actions”. We think CMMN is a better way to model this kind of flow. The algorithms will evolve over time based on evidence of health outcomes achieved. Tracking the effectiveness of these plans/interventions will also be a key role for CMMN and, moreso, BPMN-based flows.
Likewise, we like the concept of milestones in CMMN as a means to tie those sentries to behavior change stages as offered up by clinical practice guidelines.
Executable BPMN will be critical. We don’t see CMMN as standalone. We are treating CMMN as the true orchestrator as we gently creep towards using predictive models and machine learning algorithms as sentries, essentially “unlocking” optional BPMN flows based on a combination of data and operator judgement.
There was a very good document on the proposed use of BPMN and CMMN in the context of healthcare. If you are interested, let me know and I will dig it up.
I am about to leave to a conference on emergency medicine to talk to a few people and see how I can continue this line of thought. In our own houses process thinking still needs to think in a bit ;-).
Yes, I’d very much be interested in that document - good texts are rare and far between!
Here is the link to an announcement about the initiative from the OMG site. You may have already seen this. If not, click on the “Guide” link to get access to the PDF. It is 115 pages of good material. It is very encouraging to see Mayo Clinic and the US Department of Veterans Affairs involved - both very reputable institutions… and, of course, I notice screen shots of Camunda Modeler - which is also encouraging